Epigastric Hernia in Adults: Symptoms, Risks & Surgical Care
- BY Dr. Ajay Patel
- December 21, 2025
- 340 Views
This article is medically reviewed by Dr. Ajay Patel, MD, a Board-Certified Internal Medicine Physician (USA), for accuracy, clinical relevance, and adherence to current medical guidelines.
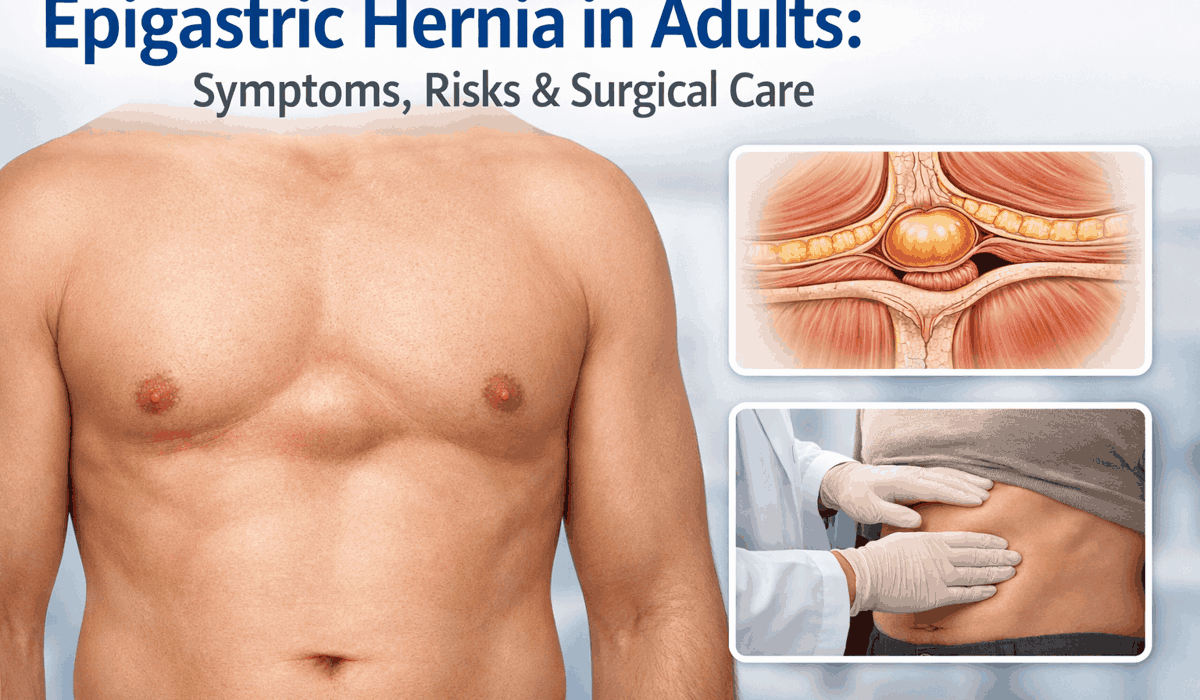
An epigastric hernia affects the upper midline of the abdomen. Adults often notice a small bulge between the breastbone and the belly button. The bulge may appear during coughing, lifting, or standing. Some people feel pain. Others feel pressure only.
This condition develops when the abdominal wall weakens. Fatty tissue pushes outward through a small defect. In adults, repeated strain plays a major role. Work demands, body weight, and chronic cough all contribute.
Early recognition helps adults decide the right next step. It also lowers fear when symptoms appear.
What is an epigastric hernia in adults?
An epigastric hernia forms along the linea alba. This structure runs down the center of the abdomen. It sits between the breastbone and the belly button. When the linea alba weakens, tissue can bulge outward.
In adults, the hernia usually contains fatty tissue. Bowel involvement remains less common. This explains why many adults report mild pain at first. Pain increases as pressure rises.
Adults often delay care because symptoms feel minor. Over time, the defect may grow. Pain may interfere with daily activity.
Why epigastric hernia is common in adults
Adult life places stress on the abdominal wall. Repeated pressure causes gradual weakening. The risk rises with age due to tissue thinning.
Common contributors include physical strain and health conditions that raise abdominal pressure. One event rarely causes the condition. Long-term stress usually does.
Main causes linked to adult epigastric hernia
These causes act over time. Awareness helps reduce future risk.
| Cause | How it affects the abdomen |
|---|---|
| Heavy lifting | Raises internal pressure |
| Chronic cough | Repeated strain on midline |
| Constipation | Frequent straining |
| Excess body weight | Constant pressure on wall |
| Pregnancy history | Stretching of tissues |
Risk factors seen in adults
Not all adults face the same risk. Some factors increase the chance of hernia formation.
Men develop epigastric hernia more often than women. Middle age shows higher rates. Previous abdominal surgery may also weaken support tissue.
Other risk factors include:
- Excess abdominal fat
- Family history of abdominal wall weakness
- Occupations involving lifting
- Reduced muscle tone with aging
Adults with multiple risk factors should watch for early signs.
Symptoms adults commonly report
Symptoms vary widely. Some adults notice only a lump. Others report pain that affects daily tasks.
The bulge often becomes visible while standing. It may reduce when lying down. Pain increases during strain.
Common adult symptoms include:
- Small bulge above the belly button
- Discomfort during lifting or bending
- Pain when coughing or sneezing
- Local tenderness
Sudden severe pain signals concern. Nausea or vomiting also needs urgent attention.
How epigastric hernia differs from similar conditions in adults
Several adult conditions resemble an epigastric hernia. Accurate distinction avoids delay in care.
Doctors rely on location and behavior of the bulge. Imaging helps when the exam feels unclear.
Comparison of upper abdominal conditions in adults
These conditions appear similar but differ in structure and risk.
| Condition | Key feature | Pain pattern | Response to strain |
|---|---|---|---|
| Epigastric hernia | Midline defect with fat | Mild to moderate | Bulge increases |
| Umbilical hernia | Bulge at belly button | Variable | Bulge increases |
| Lipoma | Soft fatty lump | Rare | No change |
| Diastasis recti | Muscle separation | None | Ridge forms |
Why adult cases need careful evaluation
Adult epigastric hernias behave differently from childhood cases. Adult tissues heal slower. Pressure remains constant due to daily activity.
Ignoring symptoms may lead to growth of the defect. Pain may limit work or exercise. Rare complications may occur if tissue becomes trapped.
Medical review helps assess risk. Doctors evaluate size, pain, and lifestyle impact. This process guides observation or surgical planning.
When observation may be reasonable
Not all adult cases need immediate repair. Small hernias without pain may remain stable. Doctors may suggest monitoring.
Observation works best when:
- Pain remains absent
- The bulge stays small
- Daily activity remains unaffected
Adults should report any change quickly. Pain progression often changes treatment plans.
Emotional concerns adults often face
Many adults worry about surgery. They fear pain or long recovery. Clear information helps reduce stress.
Modern repair methods focus on safety. Recovery often progresses smoothly. Doctors guide adults through each stage with care.
Understanding options builds confidence. Support during decision-making matters.
How doctors diagnose epigastric hernia in adults
Doctors begin with a focused physical exam. They inspect the upper abdomen while the patient stands. They may ask the patient to cough or tighten the abdominal muscles. This step raises pressure and helps reveal a hidden bulge.
During the exam, the doctor checks the bulge location. They assess size, tenderness, and firmness. They also check whether the bulge reduces when the patient lies down. Many adult epigastric hernias become clear at this stage.
If the exam does not give a clear answer, imaging helps confirm the diagnosis. Imaging also rules out other conditions that cause similar upper abdominal lumps.
Imaging tests used in adult diagnosis
Imaging plays a key role in adults. Excess abdominal fat may hide small defects. Pain without a visible bulge also needs further study.
Doctors choose imaging based on symptoms and exam findings. Ultrasound often serves as the first test. CT scans help in complex cases.
Common imaging methods and their purpose
Doctors use imaging to confirm the defect and plan care. Each test serves a specific role.
| Imaging test | What it shows | Typical use in adults |
|---|---|---|
| Ultrasound | Soft tissue movement and small defects | First test |
| CT scan | Defect size and contents | Surgical planning |
| MRI | Detailed soft tissue view | Rare cases |
What doctors assess after confirmation
After confirming the diagnosis, doctors assess risk. They consider pain level and bulge size. They also review daily activity and job demands.
Adults who lift often face higher strain. Pain during work raises concern. Doctors also review medical history, including prior abdominal surgery.
This assessment helps decide the next step. Some adults need monitoring. Others need repair.
When observation remains an option
Observation suits adults with mild symptoms. The bulge stays small. Pain remains absent or minimal.
Doctors may suggest observation when:
- The hernia does not limit activity
- Pain remains mild
- The bulge reduces easily
Patients should watch for changes. Pain increase or bulge growth changes the plan.
When surgical care becomes necessary
Surgery becomes necessary when symptoms affect daily life. Pain that limits movement signals concern. Bulge growth also raises risk.
Doctors often recommend repair when:
- Pain persists
- The bulge enlarges
- Activity becomes difficult
- Complications appear
Surgical care aims to close the defect. It also prevents future issues.
Overview of surgical care for adults
Surgeons repair the defect in the abdominal wall. They return fatty tissue to its place. They then close the weak area.
Surgeons choose the method based on defect size. Patient health and body structure also matter. Experience plays a role as well.
Two main repair methods exist. Each method suits different situations.
Open repair in adult epigastric hernia
Open repair uses a single incision. The incision sits over the bulge. The surgeon exposes the defect directly.
This method suits small defects. It allows direct closure. Recovery remains predictable.
Open repair benefits include:
- Direct access to the defect
- Short operation time
- Suitable for small hernias
Laparoscopic repair in adults
Laparoscopic repair uses small incisions. A camera guides the surgeon. This method allows a wider view of the abdominal wall.
Adults often recover faster after this method. Pain may remain lower. Hospital stay may shorten.
Laparoscopic repair suits:
- Larger defects
- Recurrent hernias
- Adults needing faster return to activity
Use of mesh in adult repair
Surgeons may place mesh over the defect. Mesh strengthens the repair. It lowers recurrence risk in many adult cases.
Mesh use depends on defect size. Tissue quality also matters. Surgeons discuss this choice with patients.
Possible mesh-related issues include fluid collection or infection. These remain uncommon with proper care.
Preparing adults for surgery
Preparation supports safe surgery. Doctors review medications. They advise on fasting and activity limits.
Adults may need:
- Blood tests
- Imaging review
- Anesthesia assessment
Clear instructions help reduce stress. Patients should ask questions during this stage.
Adult concerns about surgery
Many adults fear surgery. They worry about pain or time off work. Clear explanations help reduce worry.
Most adult repairs allow early movement. Pain control improves comfort. Doctors guide recovery step by step.
Understanding the plan helps adults feel ready.
Recovery after epigastric hernia repair in adults
Recovery depends on the repair method and overall health. Most adults begin walking on the same day. Early movement supports blood flow and reduces stiffness. Pain usually stays mild to moderate and improves daily.
Doctors provide clear discharge instructions. Adults should follow them closely. Good care supports healing and lowers risk.
Activity limits during healing
Activity limits protect the repair site. They also help tissue heal without added stress. Adults often return to light tasks within days.
Short walks help recovery. Long sitting should be avoided early. Lifting restrictions remain important during the first weeks.
Typical activity timeline after repair
These timeframes guide daily planning. Individual advice may vary.
| Activity | Usual timeframe |
|---|---|
| Walking | Same day or next day |
| Desk work | 3 to 7 days |
| Driving | When pain allows |
| Light exercise | 2 to 3 weeks |
| Heavy lifting | 4 to 6 weeks |
Pain control and incision care
Pain control supports comfort and mobility. Doctors often prescribe short-term pain medicine. Many adults switch to simple pain relief within a few days.
Incision care keeps the site clean and dry. Patients should check the area daily. Redness, warmth, or discharge needs attention.
Doctors explain shower timing and dressing changes. Following instructions reduces infection risk.
Diet and bowel care during recovery
Diet plays a role in recovery. Straining increases abdominal pressure. Soft bowel movements reduce stress on the repair.
Doctors often advise:
- Adequate fluid intake
- Fiber-rich foods
- Temporary stool softeners
Regular bowel habits support smoother healing. Adults should avoid constipation during early recovery.
Possible complications adults should know
Most adults recover without problems. Complications remain uncommon. Awareness helps early response.
Early issues may include swelling or fluid collection near the incision. Mild bruising also occurs. These usually improve on their own.
Later issues may include infection or recurrence. Nerve irritation may cause ongoing discomfort in rare cases.
Common complications and warning signs
Early recognition supports quick care.
| Complication | Warning sign |
|---|---|
| Infection | Fever, redness, discharge |
| Fluid buildup | Local swelling |
| Recurrence | New bulge at repair site |
| Nerve irritation | Persistent sharp pain |
Adults should contact a doctor if symptoms appear.
Risk of recurrence in adults
Recurrence means the hernia returns at the same site. Modern repair methods lower this risk. Mesh use often reduces recurrence for larger defects.
Risk depends on several factors:
- Defect size
- Repair technique
- Body weight
- Activity during healing
Following activity limits lowers strain. Long-term results remain good for most adults.
Returning to work and daily life
Most adults return to normal routines with time. Desk work resumes earlier than physical labor. Jobs requiring lifting need longer restrictions.
Doctors tailor guidance to job demands. Clear communication helps plan work return safely.
Exercise should resume gradually. Sudden strain may stress healing tissue. Doctors often guide safe progression.
Long-term outlook for adults
The long-term outlook remains positive. Most adults regain full activity. Pain usually resolves completely.
Healthy habits support lasting results. Maintaining healthy body weight lowers abdominal pressure. Proper lifting technique also helps.
Follow-up visits allow doctors to assess healing. They also address concerns early.
Living with an unrepaired epigastric hernia
Some adults choose observation instead of surgery. This choice suits small, painless hernias. Monitoring remains essential.
Adults should watch for:
- Increase in size
- New pain
- Reduced bulge movement
Any change requires review. Delay may lead to worsening symptoms.
Emotional well-being during recovery
Recovery affects more than the body. Adults may feel anxious about activity limits or work absence. Support helps during this phase.
Clear instructions reduce fear. Knowing what to expect improves confidence. Healthcare teams guide adults through recovery.
When adults should seek urgent care
Most adult epigastric hernias change slowly. Urgent problems remain uncommon. Still, some signs need quick medical review.
Severe pain that starts suddenly needs attention. A bulge that becomes hard and does not flatten raises concern. Nausea or vomiting with pain also matters.
Adults should seek urgent care if they notice:
- Sudden severe upper abdominal pain
- A firm bulge that does not reduce
- Redness or warmth over the bulge
- Fever with abdominal pain
- Nausea or vomiting
Prompt care lowers the risk of tissue damage. It also improves outcomes if surgery becomes necessary.
Emergency risks linked to epigastric hernia
Rare complications can occur when tissue becomes trapped. Blood flow may reduce. Pain increases quickly in such cases.
Doctors call this incarceration or strangulation. These conditions require immediate surgery. Delay increases risk.
Adults should not ignore sudden changes. Quick evaluation saves time and reduces complications.
Preventive steps for adults after diagnosis
Prevention focuses on reducing pressure on the abdominal wall. These steps help both treated and untreated cases.
Doctors often advise changes that fit daily life. Small adjustments support long-term comfort.
Helpful preventive steps include:
- Avoid heavy lifting when possible
- Treat chronic cough promptly
- Maintain regular bowel habits
- Manage body weight
- Use proper posture during lifting
These steps do not close the defect. They help limit strain and symptom progression.
How doctors guide adult decision-making
Doctors consider symptoms and daily impact. They also assess defect size and imaging results. Adult work demands matter during planning.
Observation suits some adults. Surgical care suits others. Shared decision-making helps adults feel confident.
Clear discussion improves satisfaction. It also reduces anxiety around treatment choices.
Preparing for surgery as an adult
Preparation improves safety and recovery. Doctors review medications and health history. They explain anesthesia steps.
Adults may need:
- Blood tests
- Imaging review
- Medication adjustments
Patients should ask questions during visits. Understanding the plan reduces stress.
Post-treatment lifestyle guidance
After repair, lifestyle habits matter. Healthy routines support healing and reduce recurrence risk.
Doctors often suggest gradual return to activity. Sudden strain should be avoided early. Long-term habits support results.
Good habits include:
- Balanced nutrition
- Regular light activity
- Proper lifting technique
- Weight management
These steps support abdominal wall health.
Frequently Asked Questions
What is an epigastric hernia in adults?
An epigastric hernia in adults is a defect in the upper midline abdominal wall. Fatty tissue pushes outward through this weak area. It forms a small bulge above the belly button.
What symptoms do adults usually notice?
Adults often notice a small bulge, pressure, or pain during coughing or lifting. Some feel tenderness at the site. Sudden severe pain needs urgent review.
How do doctors confirm the diagnosis?
Doctors use physical examination first. Ultrasound often confirms small defects. CT scans help in complex cases or surgical planning.
Do all adults with epigastric hernia need surgery?
No. Small and painless hernias may need monitoring only. Surgery becomes necessary when pain persists or the bulge grows.
What surgical options exist for adults?
Surgeons perform open or laparoscopic repair. They may use mesh to strengthen the repair based on defect size and tissue quality.
How long does recovery take after repair?
Most adults resume light activity within days. Heavy lifting usually needs restriction for several weeks. Recovery time depends on the repair method.
Can an epigastric hernia return after surgery?
Recurrence remains uncommon with modern repair methods. Risk depends on defect size, repair type, and activity during healing.
Is epigastric hernia dangerous?
Most cases remain mild. Rare complications can occur if tissue becomes trapped. Sudden pain or a firm bulge needs urgent care.
What activities should adults avoid after repair?
Adults should avoid heavy lifting and sudden strain during early recovery. Doctors guide activity return based on healing progress.
When should an adult contact a doctor immediately?
Seek urgent care for severe pain, vomiting, fever, or a bulge that does not reduce. Early evaluation improves safety.
Medical Disclaimer
This content provides general medical information for adults only.
It does not replace professional medical advice, diagnosis, or treatment.
Consult a qualified healthcare provider for personal medical decisions.